

Background: Diffuse large B-cell lymphoma (DLBCL) is frequently curable after frontline therapy, however, relapses can occur after achievement of a PET-negative complete remission (CR). Early detection of relapse may be associated with improved outcomes with second-line curative intent therapy or novel therapies. Controversy exists regarding the utility of post-therapy surveillance imaging which is associated with patient (pt) anxiety, radiation exposure, false-positive results, and cost. A retrospective study found that serial minimal residual disease (MRD) monitoring during DLBCL surveillance could identify pts at risk of relapse before clinical evidence of disease (Roschewski, Lancet Oncol, 2015). In this multicenter prospective study, we assessed whether a next-generation sequencing (NGS)-based MRD assay could be used for early detection of molecular relapse in DLBCL.
Methods: Eligible pts with DLBCL or high-grade B-cell lymphoma (HGBCL) who received anthracycline-containing chemotherapy were enrolled across five cancer centers. In pts who achieved a PET-negative CR, serial peripheral blood samples were obtained every 3 months (mos) and CT scans every 6 mos for 2 years (yrs) post-treatment. The clonoSEQ® next generation sequencing (NGS) MRD assay (Adaptive Biotechnologies, Seattle, WA) that leverages multiplex PCR followed by NGS to identify and track rearrangements of IgH, V-J, D-J and IgK/L loci and translocations in Bcl1/2-IgH was used. MRD positive was defined as any detectable rearrangement and MRD negative as no evidence of rearrangement. We also reported MRD positivity above the limit of detection (LOD) (observations required to have 95% reproducibility). Interim futility analysis was performed after approximately 50% of anticipated relapses occurred to assess the preliminary sensitivity of the assay. Progression-free survival (PFS) was defined as time from treatment start date to relapse or death.
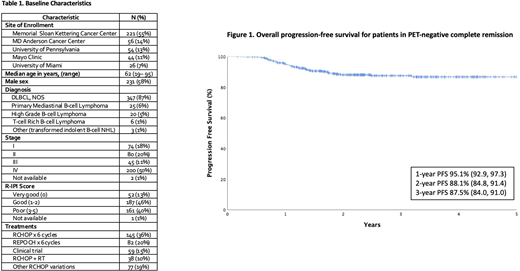
Results: 501 pts were enrolled and 401 were evaluable (pre-treatment tumor pathology available, completed frontline treatment, and achieved PET-negative CR at end-of-treatment). Baseline characteristics were median age of 62 yrs (range 19-95), male sex 58%, advanced stage 61%, and poor-risk by R-IPI 40% (Table 1). Histologies included DLBCL, NOS (86%), primary mediastinal B-cell lymphoma (6%), HGBCL (5%), T-cell rich B-cell lymphoma (1%), and other (1%). Pts received regimens including RCHOP x 6 cycles (36%), REPOCH x 6 cycles (20%), clinical trial (15%), combined modality therapy (RCHOP+RT) (10%), and other RCHOP variations (19%). Among the 401 evaluable pts, 44 relapses have occurred as of June 1, 2020. In 47% of pts (18/38), clinical relapse was detected using surveillance imaging alone (typically CT CAP with IV contrast) in an otherwise asymptomatic pt with a normal physical exam and laboratory evaluation. Clinical relapse was detected by clinical symptoms alone in 11% (4/28), by the evaluation of an oncologist alone in 0%, and by imaging and clinical symptoms and/or evaluation by an oncologist in 42% (16/38) (missing data in 6 pts). With a median follow-up of 2.2 yrs, the 2-yr PFS was 88.1% (84.8, 91.4) (Figure 1). Advanced age, advanced stage, and poor-risk R-IPI were associated with inferior PFS. Of the 44 relapses, 43 pts were included in the interim analysis and tumor-specific clonotypes were identified in 39 pts (91%). In 56% (22/39), the MRD assay was positive at or before clinical relapse. In 38% (15/39), the MRD assay was positive above the limit of detection at or prior to clinical relapse, with only 10 relapses detected more than 3 mos prior to relapse, reflecting the poor clinical sensitivity of the assay. The NGS-MRD assay was more sensitive in the acellular (plasma cell-free DNA) than in the cellular (circulating leukocytes) compartment.
Results: Overall outcomes are excellent for DLBCL and HGBCL pts who achieve PET-negative complete remission. In interim analysis, surveillance MRD assessment using the clonoSEQ® assay fails to consistently identify pts at risk of recurrence before clinical evidence of relapse in DLBCL. In a prospective analysis, a substantial proportion (47%) of clinical relapses are detected by imaging in asymptomatic pts, supporting the value of CT surveillance imaging in DLBCL, particularly for pts with advanced stage or high-risk disease. Additional analyses are forthcoming for MRD assessment in all pts, including those in remission.
Kumar:Celgene: Research Funding; Pharmacyclics: Research Funding; Adaptive Biotechnologies,: Research Funding; AbbVie: Research Funding; Seattle Genetics: Research Funding; Celgene: Honoraria, Other: Honoraria for Advisory Board; Astra Zeneca: Honoraria, Other: Honoraria for Advisory Board; Kite Pharmaceuticals: Honoraria, Other: Honoraria for Advisory Board. Westin:Kite: Consultancy, Research Funding; Curis: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Amgen: Consultancy; Astra Zeneca: Consultancy, Research Funding; Morphosys: Consultancy, Research Funding; 47: Research Funding; Janssen: Consultancy, Research Funding; BMS: Consultancy, Research Funding. Nowakowski:Curis: Consultancy; Seattle Genetics: Consultancy; Nanostrings: Research Funding; MorphoSys: Consultancy, Research Funding; Roche: Consultancy, Research Funding; Celgene/BMS: Consultancy, Research Funding; Kite: Consultancy; Denovo: Consultancy; Kymera: Consultancy; Ryvu: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other. Lossos:Verastem: Consultancy, Honoraria; Seattle Genetics: Consultancy, Other; NCI: Research Funding; Stanford University: Patents & Royalties; Janssen Biotech: Honoraria; Janssen Scientific: Consultancy, Other. Batlevi:Life Sci, GLG, Juno/Celgene, Seattle Genetics, Kite: Consultancy; Janssen, Novartis, Epizyme, Xynomics, Bayer, Autolus, Roche/Genentech: Research Funding. Drullinsky:Roche: Research Funding; Novartis: Research Funding. Gerecitano:Janssen: Current Employment. Hamlin:Celgene: Consultancy; Karyopharm: Consultancy; Juno Therapeutics: Consultancy; Portola: Research Funding; Molecular Templates: Research Funding; Incyte: Research Funding; J&J Pharmaceuticals: Research Funding; Portola Pharmaceutics: Consultancy. Horwitz:ASTEX: Consultancy; Affirmed: Consultancy; Vividion Therapeutics: Consultancy; Verastem: Consultancy, Research Funding; Myeloid Therapeutics: Consultancy; Miragen: Consultancy; Kura Oncology: Consultancy; Janssen: Consultancy; GlaxoSmithKline: Consultancy; Daiichi Sankyo: Research Funding; C4 Therapeutics: Consultancy; Beigene: Consultancy; Portola: Consultancy, Research Funding; Mundipharma: Consultancy; Innate Pharma: Consultancy; Corvus: Consultancy; Trillium: Consultancy, Research Funding; Seattle Genetics: Consultancy, Research Funding; Millenium/Takeda: Consultancy, Research Funding; Kyowa Hakka Kirin: Consultancy, Research Funding; Infinity/Verastem: Research Funding; Forty Seven: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Aileron: Consultancy, Research Funding; ADCT Therapeutics: Consultancy, Research Funding. Jacob:Adaptive Biotechnologies: Current Employment, Current equity holder in publicly-traded company. Joffe:AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Epizyme: Membership on an entity's Board of Directors or advisory committees. von Keudell:Bayer: Research Funding; Pharmacyclics: Research Funding; Genentech: Research Funding. Lahoud:MorphoSys: Other: Advisory Board. Matasar:Bayer: Consultancy, Honoraria, Research Funding; Seattle Genetics: Consultancy, Honoraria, Research Funding; Rocket Medical: Consultancy, Research Funding; Teva: Consultancy; F. Hoffmann-La Roche Ltd: Consultancy, Honoraria, Research Funding; GlaxoSmithKline: Honoraria, Research Funding; Takeda: Consultancy, Honoraria; Daiichi Sankyo: Consultancy; IGM Biosciences: Research Funding; Janssen: Honoraria, Research Funding; Pharmacyclics: Honoraria, Research Funding; Immunovaccine Technologies: Honoraria, Research Funding; Merck: Consultancy; Juno Therapeutics: Consultancy; Genentech, Inc.: Consultancy, Honoraria, Research Funding. Mullins:Adaptive Biotechnologies: Current Employment, Other: shareholder. Noy:Pharmacyclics: Research Funding; NIH: Research Funding; Rafael Pharma: Research Funding; Janssen: Consultancy; Pharmacyclics: Consultancy; Medscape: Consultancy; Targeted Oncology: Consultancy; Morphosys: Consultancy. Straus:Seattle Genetics: Consultancy, Membership on an entity's Board of Directors or advisory committees; ASH: Other: Conference in December 2019 on HL to other physicians during ASH; Elsevier: Membership on an entity's Board of Directors or advisory committees, Other: CME writer; OncLive: Speakers Bureau; Takeda Pharmaceuticals: Research Funding, Speakers Bureau; NY Lymphoma Rounds: Consultancy; Targeted Oncology: Consultancy, Speakers Bureau; Imedex, Inc.: Speakers Bureau; Karyopharm Therapeutics: Membership on an entity's Board of Directors or advisory committees. Younes:Takeda: Consultancy; HCM: Consultancy; AstraZeneca: Current Employment; Novartis: Consultancy; Daiichi Sankyo: Consultancy; Janssen: Consultancy; Epizyme: Consultancy; BMS: Consultancy; BioPath: Consultancy; Curis: Consultancy. Zelenetz:MEI Pharma: Research Funding; MorphoSys: Research Funding; Sandoz: Research Funding; Celgene: Research Funding; Roche: Research Funding; Gilead: Research Funding; Genentech/Roche: Consultancy; Gilead: Consultancy; Celgene: Consultancy; Janssen: Consultancy; Amgen: Consultancy; Novartis: Consultancy; Adaptive Biotechnology: Consultancy; BeiGene: Membership on an entity's Board of Directors or advisory committees.

